
Background:
Testosterone is mentioned often in the news and in print, but here we summarize the basics. Did you know?
– 1 in 4 men may suffer from low testosterone
– Low testosterone is a common condition affecting more than 5 million men between ages 30 and 80 years in the United States
– Testosterone levels decline by 10% every decade beginning at age 30 years
– Low testosterone is associated with:
Decreased sex drive, soft and small testes, decreased sperm count, decreased bone density and muscle mass, increased body fat, hot flashes, gynecomastia (breast enlargement) and body hair loss with decreased need for shaving of facial hair, and decreased bone mineral density (osteopenia or osteoporosis).
Symptoms of low testosterone also include tiredness, depressed mood, and reduced mental concentration. Large studies have shown that testosterone levels decline with age. In addition, conditions such as diabetes, heart disease, metabolic syndrome, obesity, HIV infection, varicocele, alcohol abuse, narcotic use (prescription pain medication), and steroid use have been associated with low testosterone.
Diagnosis:
Low testosterone is initially diagnosed by checking blood levels of free and total testosterone (produced predominantly by testes) in the morning on two occasions, luteinizing hormone (LH), follicle-stimulating hormone (FSH) which are both from part of the brain called the pituitary, estradiol, and inquring about patient symptoms. According to most US national guidelines, total testosterone levels below 300-350 nanograms per deciliter (ng/dl) are considered diagnostic for hypogonadism but must be interpreted along with patient symptoms. The normal range of serum total testosterone is 300-800 ng/dl (ideal levels lie between 600 and 800 ng/dl). Prior to initiation of any testosterone replacement, prostate specific antigen (PSA, a marker for prostate cancer) and blood count (hematocrit) should be checked since these may indicate possible contraindications to treatment. By checking hormone levels, it can be determined whether low testosterone can be categorized as primary (testicular issues) or secondary (brain- hypothalamus or pituitary) hypogonadism.

Treatment:
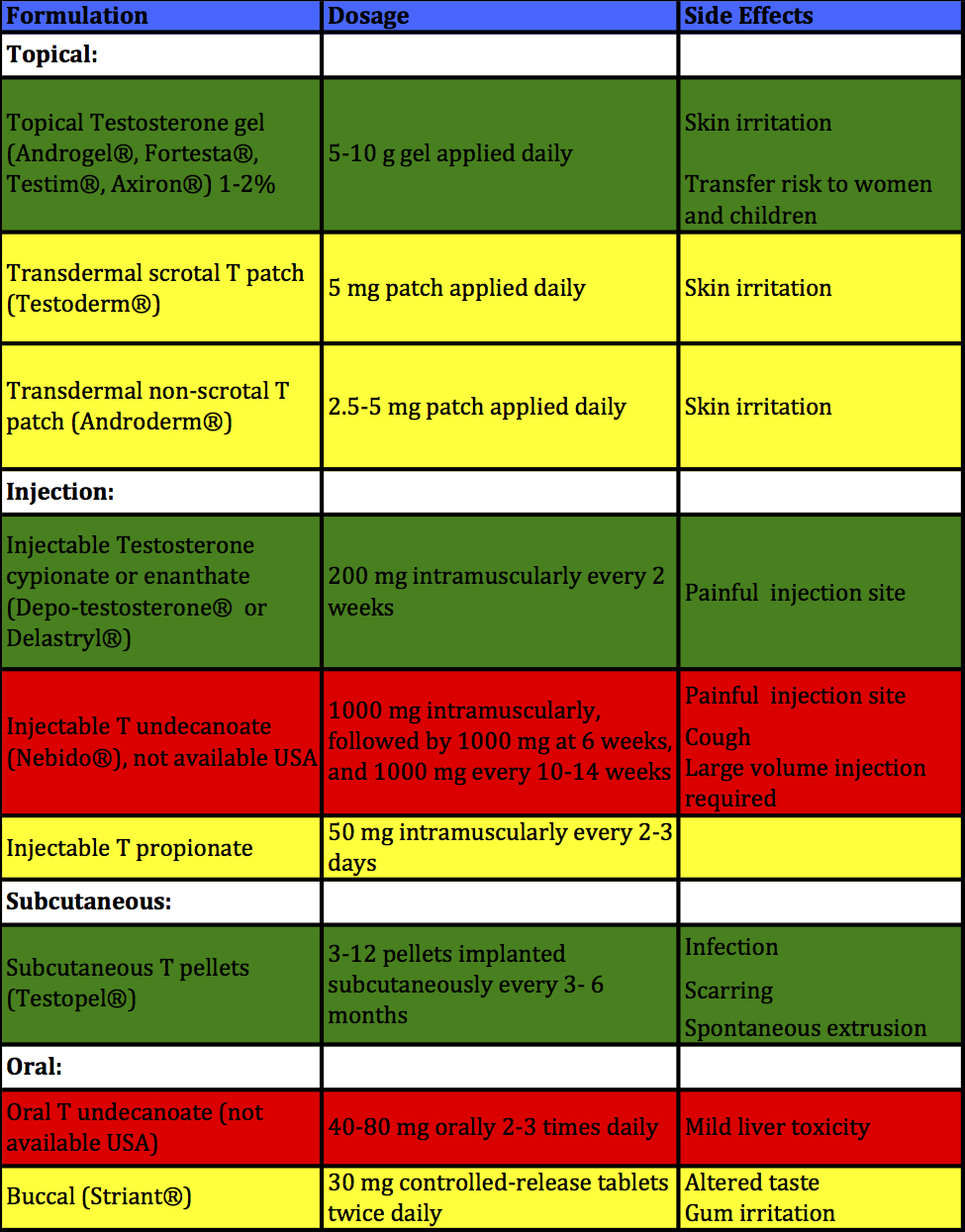
The goal of testosterone replacement therapy (TRT) is increase the daily circulating levels of testosterone to be within the normal reference range. One option is using testosterone (which provides the missing end product) for men not interested in fertility. Alternatively, if a man desires fertility preservation, then alternative medications may be used (including HCG, clomiphene citrate, recombinant LH, pulsatile GnRH) which stimulate testosterone production through the normal physiologic pathways by providing increased “fuel” normally produced by the brain (called LH and/or FSH). TRT using exogenous testosterone has been approved by the FDA since 1973. There are several approved options available using 5 different routes of administration for the treatment of androgen deficiency, including oral, buccal adherent tablets, transdermal (gels, solutions, patches), injectable, and implantable formulations of testosterone. See Table below for summary of these options.
Topical testosterone:
95% of men receiving hypogonadism treatment receive transdermal or injectable testosterone. Transdermal topical (applied on and absorbed across the skin) medications include:
Androgel 1%®, Androgel 1.62%®, Testim® (each applied daily to shoulders and upper arms to the area covered by a T-shirt), or Androderm
Fortesta® (applied daily to front/inner upper thighs)
Axiron® (applied daily to underarms)
The exact dosage is determined and adjusted based on your baseline serum testosterone and and follow-up values. Transdermal preparations achieve normal testosterone levels in up to 87% of men, but require daily application in the early morning to clean dry skin after showering, and adequate (up to 5 minutes) drying time. Following skin application, the steroid is rapidly absorbed into the stratum corneum (part of the skin), which forms a storage reservoir and acts as a rate-controlling area to deliver testosterone continuously over a 24-hour period. All topical formulations have potential for transference to women and children (increased hair in women, and irreversible bone changes in children) and may cause skin reactions. Long-term studies of testosterone gels are safe and with good results raising testosterone to the normal range. As an alternative to gels, topical patches either using scrotal (Testosderm®) or non-genital skin (Androderm®) also cause skin reaction.
Injectable testosterone:
Injectable intramuscular testosterone include include testosterone propionate (short-term forumation requiring dosing often: every 2-3 days, and therefore is not widely used). Testosterone cypionate (Depo-testosterone®) and testosterone enanthate (Delatestryl®) are administered 100-200 mg every 2-4 weeks and are the most commonly used due to low cost and long-term safety records. Testosterone undecanoate (Aveed® in USA, Nebido® in internationally) is a long-lasting testosterone administered intramuscularly, with an initial loading dose followed by a second dose at 6 weeks, and additional doses every 10-14 weeks thereafter). The advantage of all injection treatments is avoiding the requirement of daily use and the transfer risk to women and children. Following injection, serum testosterone (T) reaches supraphysiologic levels after 24 hours, followed by a gradual reduction to baseline T levels over the following 2 weeks. As a result, patients experience fluctuating high and low serum T levels, which may be paralleled by their symptoms. At the initiation of therapy, peak and trough serum T levels drawn 24-48 hours after and before administration respectively to guide dose or dosing interval adjustment. Lower doses at more frequent intervals help minimize fluctuations in serum T. Alternatively, for patient ease, T levels may be checked midway between injections. While there may be more predictable delivery of testosterone with injection than transdermal application, there is a slightly increased risk of elevating the blood count too high with injectable when compared to topical testosterone.
Other routes of testosterone:
The longest-lasting choice for TRT is the subdermal implantation of pellets (Testopel®) made of crystallized testosterone. Each pellet contains 75 mg of T, and typical dosing starts at 3-6 pellets (up to 12 pellets) placed every 3 to 6 months to achieve normal T levels. Pellets may be implanted in the lower abdominal wall, buttocks, or upper thighs. Pellet implantation is a 10-15 minute office-based procedure, performed using local anesthesia. Pellets should only be used in patients who have already shown a benefit from TRT. Disadvantages include rare adverse local effects such as extrusion, bleeding, infections, and fibrosis.
In addition, testosterone nasal gel (Natesto®) is available and is used three times daily to each nostril. Oral testosterone (Testosterone undecanoate, Jatenzo®) is available in the United States. Trans-buccal testosterone (30 mg buccal tablet, Striant®) which adheres to gum or inner cheek in mouth has been shown to result in similar T level compared to T gel but may lead to gum irritation in 20% of men. The table below summarizes the most common testosterone replacement routes used (green), other options (yellow), and those not available in the United States (red).
Treatment of Low Testosterone in Men Desiring Children:
Any of the testosterone preparations discussed so far will have very negative effects on sperm, semen quality (azoospermia is possible), and male fertility. These effects can linger for months or even years after stopping testosterone. For men interested in fertility, see this post regarding treatment for men with low testosterone who want to protect their fertility to have children in the future.
Benefits of Raising Testosterone:
The benefits of raising testosterone to normal levels includes improvement in energy, strength, sexual function, body composition (increased lean body mass, decreased fat mass), bone mineral density, decreased diabetes, cholesterol and heart issues, mood, and cognition in men of all ages. More trials are needed to establish benefits and adverse effects of testosterone replacement therapy (TRT). Risks of treatment include acne, increased male pattern baldness, gynecomastia, decreased spermatogenesis, worsened prostatic enlargement and difficulty urinating (AUA symptom score). Stopping testosterone typically reverses these side effects in most men. Serious risks of TRT include development or acceleration of prostate or breast cancer, but the prostate cancer risk has not been supported by current available studies and TRT is being used in some patients with a history of prostate cancer at certain centers. Men with elevated PSA or abnormal prostate exam, or recent heart issue in past 6 months such as heart attack or congestive heart failure require further evaluation before any consideration of treatment. While the majority of studies show that TRT is beneficial and safe in older men even those with cardiovascular issues, there are four recent studies which question the safety of TRT in terms of cardiovascular outcomes. However, there are some major flaws in these studies, so additional work is needed to determine the use of TRT in men with cardiovascular issues. Other risks of TRT include liver toxicity (with oral testosterone), increased blood count, worsening of sleep apnea (abnormal breathing during sleep), worsening of heart failure, and decreased “good” HDL cholesterol in blood.
Follow-up:
Once the patient initiates treatment for low testosterone, patients’ serum testosterone should be checked (always before 10 AM for accuracy) every 2 weeks at initiation of therapy and with dosage change. Then men should be evaluated 3-6 months following the initiation of therapy, and then annually, to determine symptom response, serum total testosterone (and free testosterone in certain cases) as well as any adverse outcomes. Serum total testosterone should remain in the mid-normal range (ideally 600-800 ng/dl), and hematocrit (blood count), PSA, and bone mineral density (every 1-2 years) with DEXA scan should be monitored. The appropriate management of low testosterone is clearly critical for male health and must be customized by discussion between patient and physician.
We are pleased to discuss low testosterone diagnosis and associated symptoms of hypogonadism and low testosterone with you. Please contact us for additional information and to schedule a consultation.
- Low testosterone may cause multiple symptoms including tiredness, reduced concentration, decreased sex drive, lower sperm count, decreased bone density and muscle mass, hot flashes, breast enlargement and body hair loss.
- Low testosterone may result for many reasons, along with a general decline in testosterone which occurs with age.
- The potential benefits and risks of testosterone replacement must be carefully considered based on the most recent body of medical literature.
- At CMHR of Connecticut, we collaborate with physicians from many disciplines including endocrinology and cardiology to treat low testosterone and its consequences.

